My Response to the Medical Board
Ironically, despite having recognized the dangers of overreliance on opioids in the early 2000's and working for nearly 2 decades to help patients find effective alternatives, I am being censured as negligent and as an "overprescriber" because I did not simply cut off patients who were not able to safely taper off their medications as quickly as the state would like. As people who know my work ethic and availability to my patients, you know that what I do is the opposite of negligence, though of course there are decisions I agonize over, like any doctor.
With regard to my care of a breadth of patients who suffer with intractable chronic pain, a look at my record since 2003 in addressing pain management with a holistic, non-opioid-centered approach, will underscore that I am the fireman, not the arsonist, in this situation. I have helped a great number of patients to decrease their dependency on opioids, or to get off of them completely, and I've helped a number to learn to live more satisfying lives despite chronic pain, sometimes with the help of these medications but without them as their sole treatment modality.
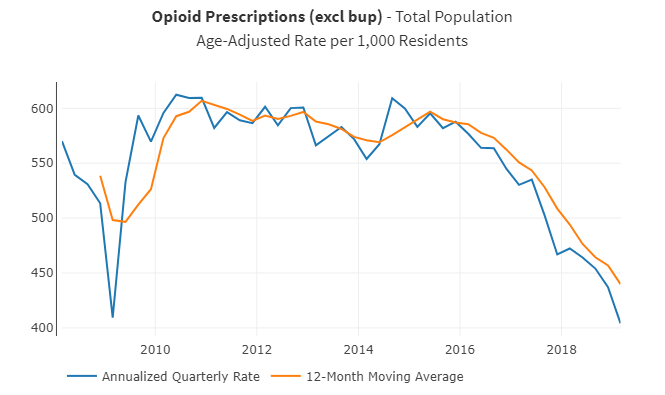
The following graphs demonstrate what the current "standard of care" in California is accomplishing. The 2014 guidelines and pattern of prosecuting physicians since 2016 has indeed led to a decrease in opioid prescriptions:
And the results? The "success" of the policy appears to have increased overdose deaths.
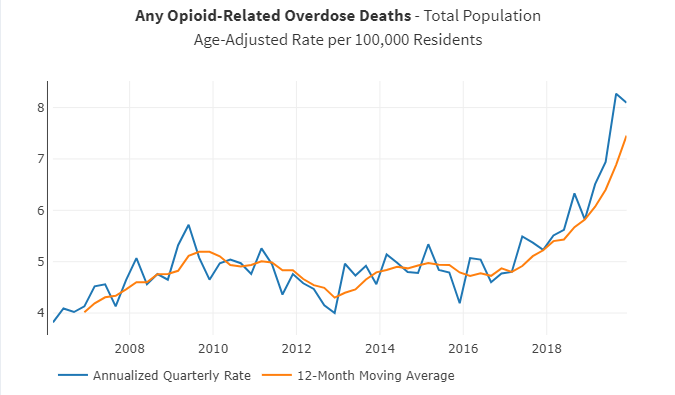
Reports state these numbers are even worse during the pandemic, though no official statistics are yet available.
Correlation does not prove causation, but I have a number of case histories that demonstrate the mechanisms by which this may be occurring. I resisted the previous Medical Board Guidelines in the early 2000's as well: while they were telling physicians to use MORE opioids, I required patients to come to educational support groups in order to get their medications, encouraged alternatives, etc. Now the Board tells physicians to use less, but I believe the middle path remains the correct one. People in pain, and who were hooked on these medications by doctors following those previous Guidelines, do not do well when forced to taper opioids against their will and despite their objections.
These patients face the competing risks of suicide, alternative/illicit opioid-seeking in order to manage their pain, and significant loss of function if they are left without care.
The federal government has recognized this, which is why recent (2019) clarifications from CDC") , FDA, and HHS all have cautioned against nonconsensual tapers of chronic or "legacy" pain patients. Recent studies in Washington, Colorado, and Vermont document increased overdoses and hospitalizations related to policies which encourage forced tapers. There is also a case series of more than 500 patients who have committed suicide in response to loss of access to pain management which has been collated by Anne Fuqua, RN (even this is believed to be a substantial undercount.)
, FDA, and HHS all have cautioned against nonconsensual tapers of chronic or "legacy" pain patients. Recent studies in Washington, Colorado, and Vermont document increased overdoses and hospitalizations related to policies which encourage forced tapers. There is also a case series of more than 500 patients who have committed suicide in response to loss of access to pain management which has been collated by Anne Fuqua, RN (even this is believed to be a substantial undercount.)
Due to my Hippocratic oath, I cannot follow guidelines which cause this kind of harm. I was scolded by the judge at a prehearing settlement conference for "not showing remorse" for using my best clinical judgment, and for being unwilling to commit to follow those guidelines in the future. I reject this attempt to shame me for doing my very best as a physician for my patients, but I expect they are going to continue to attempt to shame me.
So, Medical Board, while I respect your mission to protect patients in California: "SHAME ON YOU."
2. Lumping the diligent, compassionate physicians - the ones who are trying to help people who are trapped - in with “pill mill” docs who cynically profiteered by getting them hooked in the first place. This careless harassment represents a failure of investigative function. I know of other doctors in Northern CA who practice like I do who are facing similar issues - you are attacking those of us who are trying to help these desperate patients.
3. Claiming to address the "opioid epidemic" without acknowledging that 2/3 of overdose deaths are from illicit fentanyl and other synthetic opioids. You are shutting down the wrong supply and depriving vulnerable patients of their access to needed medical care.
And furthermore, shame on you for wasting enforcement resources on my practice while failing to protect our community from other physicians who were either serial sexual offenders or actively abusing substances, etc. Shame on you for treating my dissent as "misconduct" while failing to appropriately prevent the egregious misbehavior of impaired colleagues, with sham probation that did not mandate rehabilitation for them.
I have a particular bristle with the "you have too soft a heart" criticism: there is something the matter with a caring profession where caring is deemed a shortcoming. Why is contempt and judgment for the actual people we serve being held up as the standard? Why are we being encouraged to cut patients off and refer them to substance abuse care (even when their diagnosis is chronic pain, not substance use disorder) without anyone looking at the dismal results of that sort of approach? I could provide a tour of downtown Eureka to show how well that is working out around here. . . .
I think we all, as human beings, deserve compassionate medical care at all times, no matter who we are, where we live, what our finances, what our background, or even what our behavior. I will say that for my patients who have misused their medications, and for those who have overeaten or continued to smoke or in some other way shown human failing, and even for those thoughtless people who have implemented policies that have harmed others.
, and find that I cannot locate the phrases that state:
• I will ensure that punishment occurs when patients violate agreements
• I will reveal patients' innermost secrets to governing agencies, insurance companies, and the general public
• I will endorse patient suffering if it protects my income, career goals, and personal well-being
I am sorry for the amount of disruption that this has caused and will cause to my other patients, but I believe we will be judged by how we have cared for those who are most vulnerable.(below) Those with chronic illness and particularly chronic pain have been stigmatized and scapegoated in recent years, even systematically abandoned by much of my profession (wisely, clearly, for the sake of their own licenses.) For me, this was a moral line that I could not cross.
Connie Basch, MD
"The test of a civilization is the way that it cares for its helpless members.” Pearl Buck
“A Nation should not be judged by how it treats its highest citizens, but its lowest ones” Nelson Mandela
Please contact:
The Medical Board of California 1-800-633-2322 complaint at mbc.ca.gov
Assembly member Jim Wood 707-445-7014 https://a02.asmdc.org/
State Senator Mike McGuire 707-445-6508 https://sd02.senate.ca.gov/ mike.mcguire at senatormikemcguire.com
Governor Gavin Newsom 916-445-2841 https://govapps.gov.ca.gov/gov40mail/
Ask them to
1. Review the actions of the Medical Board, the Guidelines for Treatment for Chronic Pain, and ask how the medical board is revising policies in light of emerging data on the harm the policies are causing. Ask if they are reexamining the cases in the pipeline to distinguish pill mill docs from those trying to care for the opioid refugees.
2. Ask if they are addressing the access problems of patients in underserved communities - in our community, of 20 practices surveyed, only one said they would accept new patients with chronic pain or chronic opioid use other than suboxone.
3. Ask why the Board is censuring respected local physicians in health provider shortage areas. Is it for the protection of the public? How do they calculate that?
If you know reporters with a state or national platform, encourage them to ask the same questions..
Consider joining https://dontpunishpainrally.com/, California group
Another article analyzing the unintended consequences of the Anti-opioid crusade:
CDC Analyzes Deaths Caused By Its Own Anti-Opioid Crusade
With regard to my care of a breadth of patients who suffer with intractable chronic pain, a look at my record since 2003 in addressing pain management with a holistic, non-opioid-centered approach, will underscore that I am the fireman, not the arsonist, in this situation. I have helped a great number of patients to decrease their dependency on opioids, or to get off of them completely, and I've helped a number to learn to live more satisfying lives despite chronic pain, sometimes with the help of these medications but without them as their sole treatment modality.
The following graphs demonstrate what the current "standard of care" in California is accomplishing. The 2014 guidelines and pattern of prosecuting physicians since 2016 has indeed led to a decrease in opioid prescriptions:
And the results? The "success" of the policy appears to have increased overdose deaths.
Reports state these numbers are even worse during the pandemic, though no official statistics are yet available.
Correlation does not prove causation, but I have a number of case histories that demonstrate the mechanisms by which this may be occurring. I resisted the previous Medical Board Guidelines in the early 2000's as well: while they were telling physicians to use MORE opioids, I required patients to come to educational support groups in order to get their medications, encouraged alternatives, etc. Now the Board tells physicians to use less, but I believe the middle path remains the correct one. People in pain, and who were hooked on these medications by doctors following those previous Guidelines, do not do well when forced to taper opioids against their will and despite their objections.
These patients face the competing risks of suicide, alternative/illicit opioid-seeking in order to manage their pain, and significant loss of function if they are left without care.
The federal government has recognized this, which is why recent (2019) clarifications from CDC
Due to my Hippocratic oath, I cannot follow guidelines which cause this kind of harm. I was scolded by the judge at a prehearing settlement conference for "not showing remorse" for using my best clinical judgment, and for being unwilling to commit to follow those guidelines in the future. I reject this attempt to shame me for doing my very best as a physician for my patients, but I expect they are going to continue to attempt to shame me.
So, Medical Board, while I respect your mission to protect patients in California: "SHAME ON YOU."
Shame on you for distraction:
Shame on you for distracting me during a Public Health Emergency (Covid-19) with a counterproductive approach to another public health emergency (the illicit opioid epidemic.)Shame on you for misdiagnosis:
1. Confusing people with chronic intractable pain with addicts seeking drugs.2. Lumping the diligent, compassionate physicians - the ones who are trying to help people who are trapped - in with “pill mill” docs who cynically profiteered by getting them hooked in the first place. This careless harassment represents a failure of investigative function. I know of other doctors in Northern CA who practice like I do who are facing similar issues - you are attacking those of us who are trying to help these desperate patients.
3. Claiming to address the "opioid epidemic" without acknowledging that 2/3 of overdose deaths are from illicit fentanyl and other synthetic opioids. You are shutting down the wrong supply and depriving vulnerable patients of their access to needed medical care.
Shame on you for failing to monitor:
Shame on you for Shame on you for enacting Pain Management policies and not monitoring the outcome of those policies.Shame on you for missing the red flags:
Shame on you for missing the red flags of increased overdoses and suicides in response to your policy, and failing to change your approach even after federal guidelines have been issued to warn of the risks.Shame on you for contributing to physician burnout:
Shame on you for policies that have encouraged uncompassionate behavior among my colleagues, who are intimidated into ignoring their own clinical instincts.Shame on you for avoiding meaningful debate:
Shame on you for making this a legal matter rather than a peer review matter, where differences in opinion and practice could be debated and your harmful interpretation of the guidelines could actually be challenged.Shame on you for targeting those less able to fight back:
Shame on you for coming after me and others who are serving underserved populations and therefore earning less money, or who are nearing retirement age and who therefore cannot spend the money on lawyers to defend their good names. My income here is 1/3 what it was when I worked at the Residency in Washington. I am told my defense at a hearing would have cost more than 2 years' income, a dubious investment when I am 57 years old.Shame on you for sampling errors:
Shame on you for sampling only my most challenging patients, the ones who others would have fired but who I stuck with and kept working with, using professional judgment and perseverance to help them along their healing journeys. By refusing to look at my overall pattern of practice and my accomplishments, you failed to see the many patients who have tapered medications and resumed functioning in the world and their families, or to even note the cases that I have had to discharge or transfer to buprenorphine because I did recognize safety issues with continued prescribing. You have accused me of failing to respond appropriately to red flags, but failed to notice that my outcomes have actually been good, without the high number of patients discharged and lost to care who contribute to the worst poor outcome statistics in our state and the increase in deaths.Shame on you for incentivizing patient abandonment:
Shame on you for incentivizing doctors to write people off as disposable rather than deal with the messy hard work of trying to help traumatized and struggling people become or remain stable.Shame on you for poorly targeted Enforcement activities:
Shame on you for offering me a probation deal that clearly reveals that you know that my prescribing does not endanger the public, but nevertheless requires me to be punished and defamed for providing the best care I am able.And furthermore, shame on you for wasting enforcement resources on my practice while failing to protect our community from other physicians who were either serial sexual offenders or actively abusing substances, etc. Shame on you for treating my dissent as "misconduct" while failing to appropriately prevent the egregious misbehavior of impaired colleagues, with sham probation that did not mandate rehabilitation for them.
I have a particular bristle with the "you have too soft a heart" criticism: there is something the matter with a caring profession where caring is deemed a shortcoming. Why is contempt and judgment for the actual people we serve being held up as the standard? Why are we being encouraged to cut patients off and refer them to substance abuse care (even when their diagnosis is chronic pain, not substance use disorder) without anyone looking at the dismal results of that sort of approach? I could provide a tour of downtown Eureka to show how well that is working out around here. . . .
I think we all, as human beings, deserve compassionate medical care at all times, no matter who we are, where we live, what our finances, what our background, or even what our behavior. I will say that for my patients who have misused their medications, and for those who have overeaten or continued to smoke or in some other way shown human failing, and even for those thoughtless people who have implemented policies that have harmed others.
Why I settled:
This probation deal says I can never, at a hearing in the future, legally dispute the charges of the Accusation, which is riddled with inaccuracies and is defamatory to me and my patients. As one example, a reviewer interpreted the abscess caused by a cat scratch from a rescue cat as clear evidence of intravenous drug abuse in someone who does not inject drugs, then accused me of failing to recognize and act on this imaginary red flag. Nonetheless, in order to dispute this, I was being asked to spend more than 2 years' salary on legal expenses, just for the opportunity to have a remote hearing over the internet, with glitches and screen freezing, and without my patients as witnesses to testify on my behalf. The only way I could have had patients present as witnesses would have involved asking them to break their doctor/patient confidentiality and reveal their identities and medical matters to the public, and though a number volunteered for that, I was not comfortable allowing it to occur.My Oath:
I recently listened again to the oath that I took upon graduation• I will ensure that punishment occurs when patients violate agreements
• I will reveal patients' innermost secrets to governing agencies, insurance companies, and the general public
• I will endorse patient suffering if it protects my income, career goals, and personal well-being
I am sorry for the amount of disruption that this has caused and will cause to my other patients, but I believe we will be judged by how we have cared for those who are most vulnerable.(below) Those with chronic illness and particularly chronic pain have been stigmatized and scapegoated in recent years, even systematically abandoned by much of my profession (wisely, clearly, for the sake of their own licenses.) For me, this was a moral line that I could not cross.
Connie Basch, MD
"The test of a civilization is the way that it cares for its helpless members.” Pearl Buck
“A Nation should not be judged by how it treats its highest citizens, but its lowest ones” Nelson Mandela
If you want to do something about this:
If you have any available bandwidth in the midst of the economic and public health crisis of the pandemic, help me make sure they come to know what they do. Our legislators cannot intervene in my particular case, but they can be asked to address this policy of aggressive prosecution of doctors who have accepted the opioid refugees.Please contact:
The Medical Board of California 1-800-633-2322 complaint at mbc.ca.gov
Assembly member Jim Wood 707-445-7014 https://a02.asmdc.org/
State Senator Mike McGuire 707-445-6508 https://sd02.senate.ca.gov/
Governor Gavin Newsom 916-445-2841 https://govapps.gov.ca.gov/gov40mail/
Ask them to
1. Review the actions of the Medical Board, the Guidelines for Treatment for Chronic Pain, and ask how the medical board is revising policies in light of emerging data on the harm the policies are causing. Ask if they are reexamining the cases in the pipeline to distinguish pill mill docs from those trying to care for the opioid refugees.
2. Ask if they are addressing the access problems of patients in underserved communities - in our community, of 20 practices surveyed, only one said they would accept new patients with chronic pain or chronic opioid use other than suboxone.
3. Ask why the Board is censuring respected local physicians in health provider shortage areas. Is it for the protection of the public? How do they calculate that?
If you know reporters with a state or national platform, encourage them to ask the same questions..
Consider joining https://dontpunishpainrally.com/
Another article analyzing the unintended consequences of the Anti-opioid crusade:
CDC Analyzes Deaths Caused By Its Own Anti-Opioid Crusade